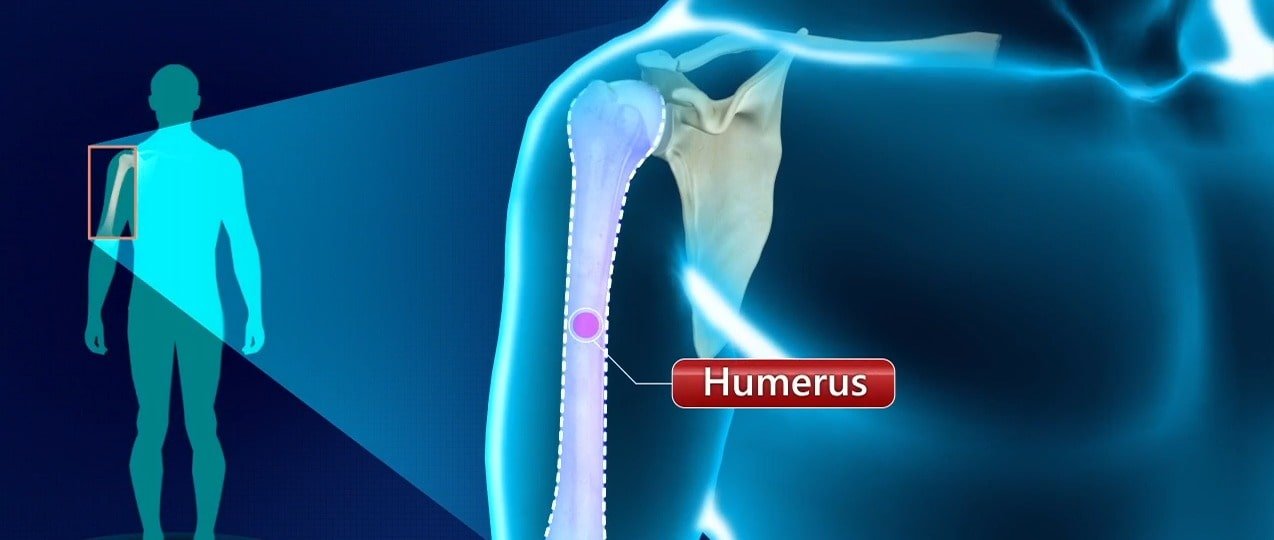
In this case study, we would like to discuss the management of the closed fracture of the humerus.
The primary step involved in the treatment of a closed fracture of the humerus (long bone in the upper arm) by orthopedic implants doctor involves stabilization of the extremity in either coaptation splints (A short strip of rigid material used for supporting and is designed in a way to prevent overriding of the ends of a fractured bone of the entire limb), hanging casts, or slings in order to provide soothe and correct major fracture deformities.
Extreme situations like a fracture that involves the manipulation of a humeral fracture to obtain sufficient alignment of the fragments are very rare occurrences. The orthopedic instruments research department quotes that manipulation, if highly required, then only should be done. Also, it should be done very cautiously so as to avoid any damage to the peripheral nerves, particularly the radial nerve, which is the most susceptible.
Nerve paralysis that develops following the treatment of humeral fracture with manipulation usually has a worse medical experience than when it occurs at the time of injury. In the latter instance, i.e. during the time of injury, the nerve tremor is basically due to a bruise or accident and therefore spontaneous recovery is possible. Another analysis done by our Orthopedic Implants Manufacturers company has also stated that the occurrence of radial palsy in comminuted butterfly fractures of the distal third of the humerus is high. In such cases, we believe that surgical exploration is routinely not so necessary.
Furthermore, our orthopedic implant company list in India report also suggested not using “cock-up” dorsiflexion splints (A pre-shaped and molded palm splint made of light metal that maintains flexion of the foot in the dorsal, or upward, direction) for the wrist, as their presence, rather than being helpful, maybe unfavorable with respect to limiting the patient’s movements of the hand. It is also important to note that providing support to the limb using braces requires an early extension of the elbow and further dependency on the extremity which further brings the wrist to a neutral attitude and therefore, prevents muscle stiffness or contracture.
As leading orthopedic implant manufacturers in India, we believe that it is advantageous to introduce pendulum exercises to the shoulder as soon as the acute symptoms caused by the humeral fracture subside. Early exercises prevent the development of disabling adhesive capsulitis (a condition in which ligaments surrounding the joint at the base of the second toe have become inflamed), which, particularly in the elderly, may cause disability for a period of time longer than that required for therapeutic of the fracture. The physiotherapist at our orthopedic implants suppliers office quotes that in addition to the shoulder exercises, the active motion of the forearm and hand is suggested since it appears that these exercises accelerate the overall revival and lessening of swelling.
Presently, it is possible to apply the functional sleeve within 1 week of the initial injury. However, if there is substantial swelling of the arm away from the torso, it is best to hold up the application of the sleeve. During this period of holdup or wait, pendulum exercises must be sustained (to and fro motion of the hand on support like a table), and passive motion of the elbow should be done whenever possible.
Sleeves designed by our orthopedic implant manufacturers fits snugly over the arm. Another type of sleeve used in such cases is a collar-and-cuff sling. During the application of the collar and cuff sling, it is important to take into account that the shoulder is not shrugged. If the collar-and-cuff sling is applied in a shrugged shoulder, an angular deformity of the humerus could take place upon relaxation of the shoulder muscles. The sleeve must, as indicated previously, must fit in a warm and comfortable manner but not so much as to squeeze venous return which may result in swelling and disability of the distal arm.
In our orthopedic implants India office, the sleeves are made of plastic material in order to be adjustable. The rapid reduction of swelling and the development of weakened muscles reduce the girth of the arm and the sleeves are displaced distally. Such displacement requires frequent adjustments, which can be made by the patient after appropriate only if the sleeves are adjustable. It is important to note that the sleeve does not necessarily have to be extended above or below the fracture since the firmness of the soft tissues and gravity can adequately provide the desired position of the fracture. As soon as the sleeve has been applied, pendulum exercises should be brought into action. The orthopedic implants patient should frequently remove the arm from the sling and exercise actively and passively against the elbow joint in order to gradually regain range of movement.
It is advantageous to regain full extension of the elbow during the initial week of the application of the functional sleeve. If not regained early, chances of correction of deformities greatly reduce and lead to the creation of anterior angular abnormalities. Active and passive movement should be done as soon as possible.
Our trauma implants and Spine Implants physiotherapist also states that once the patient has been able to extend the elbow and the chances of increased swelling distally getting reduced, the collar-and-cuff sling can be removed and the pendulum exercises should be carried out as per the instruction. Also, in these cases, the sling is recommended only during sleep ours at night.
Any delay in retrieval elbow extension is likely to cause an anterior apex angular deformity at the fracture site. The muscle stiffness that has developed at the elbow joint during the period of immobilization of the joint transfer trauma to the fracture site that leads to further deformity. In such cases, trauma implants doctors prevent any kind of seizure and elevation exercises until full-grown bone healing has taken place. Any forceful attempt to raise the arm may result in the expansion and upholding of the angular deformity. Also, it is seen in most instances that patients can regain almost full range of motion of the shoulder and elbow prior to removal of the sleeve.
Our orthopedic implant company medical specialists do not recommend functional bracing for patients who are unable to move or are bedridden. In such cases, it is best to hold the arm against the chest with a Velcro shoulder sling until the early inherent stability of the body has developed. At that time and upon confirmation after examination, the sleeve can be applied to the traumatized area.
Also in these cases, it is advisable for patients to suspend the arm over the side of the bed in order to maximize the beneficial effects of gravity. Flaccid elbow exercises can also be conducted in that fashion. In another case of women with large breasts, there are chances to develop a Varus deformity (inward angulation) at the fracture site, if the arm is held in a sling or cast and rests over the prominent breast. This is because in such cases the breast functions as a pivot where the deformity develops. The functional sleeve allows additional room for the elbow, and in such a manner the broken end falls behind the large breast and thus is not subjected to the fulcrum effect.
We also advise patients to not rest with the elbow on their laps or over hard surfaces as it has been seen that leaning on the elbow is the most common cause of any kind of angular deformity like varus or valgus.
In the treatment of open fractures of the humerus, it is important to note to a physician that the sleeve can be applied once the sensitive symptoms have reduced, even though the wound, which has been left open, may still be seeping and oozing. The proper application and removal of orthopedic instruments like the brace make it possible to carry out appropriate and frequent changes in wound dressings.
Our analysis of the orthopedic implant company report based on the analysis at two hospitals in large urban areas of the United States has given us significant opportunities to manage fractures caused by gunshot projectiles. As opposed to initial thought, the healing of comminuted fractures produced by low-velocity guns is consistent and the resulting deformities are also negligible. Local cleansing of the wound and the administration of antibiotics should be sufficient enough to heal the wound.
In cases of stern soft tissue injury, as in the case of high-velocity gun wounds, the fractured bones can be stabilized with an external fixator used for limb lengthening for a few weeks. Surgical removal of unhealthy tissue to promote healing is necessary. Once the inherent stability of the body has developed through soft tissue healing, the fixator can be removed and the limb stabilized with a brace to allow for function.
It is not unusual to see subluxation ( subluxation joint is where a connecting bone is partially out of the joint) of the shoulder joint following metaphyseal or diaphyseal humeral fractures. A clear explanation for this phenomenon by ortho surgical implants specialist is not yet available. It has been suspected that this can be due to temporary axillary nerve paralysis, but in the great number of such cases, no neurological deficit can be determined.
The reason for the connecting bone of the shoulder getting out of the joint is due to a temporary loss of the muscles around the shoulder, states an orthopedic implant company researcher. In the absence of muscle quality, the weight of the extremity brings about a distal dislocation of the humeral head in relation to the glenoid fossa. This subluxation or removal of connecting bone out of the joint corrects itself spontaneously after the implementation of the functional activity of the extremity. The most effective way to overcome this is by the introduction of the early contraction movement of the biceps and triceps muscles. Active movement of the biceps and triceps leads to early initiation in comparison to the deltoid muscle. Furthermore, active seizure and elevation of the shoulder before firm stability of intrinsic fracture are not supported by orthopedic implants specialists.